
ROI Analysis: When to Upgrade from Analog to Digital Radiography
Article Summary
The Financial Imperative: Why Hospitals are Transitioning to DR For hospital C-suite executives and healthcare private equity investors, medical imaging is...

The Financial Imperative: Why Hospitals are Transitioning to DR
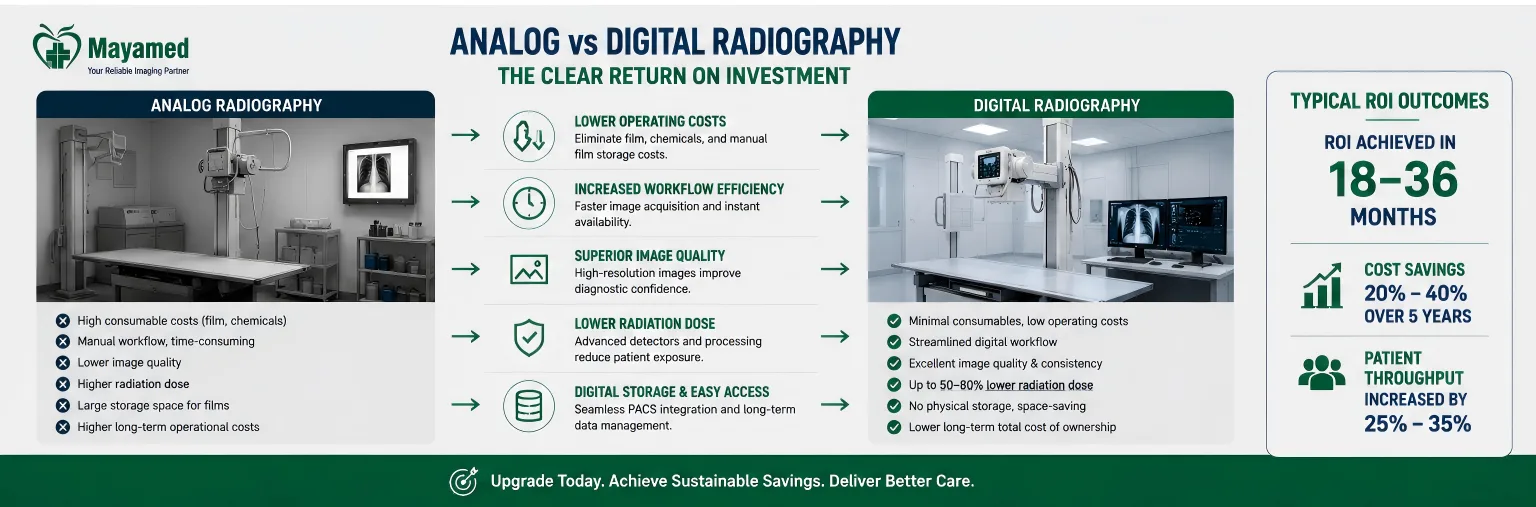
For hospital C-suite executives and healthcare private equity investors, medical imaging is no longer just a clinical cost center; it is a critical lever for operational efficiency and margin preservation. The transition from analog film-based radiography to digital radiography (DR) represents a fundamental shift in healthcare asset management. While the clinical advantages of DR—such as superior image quality and dose reduction—are well documented, the financial catalyst driving modernization is the urgent need to optimize Total Cost of Ownership (TCO) and align with value-based care mandates.
Continuing to operate analog radiography suites in the current economic climate is a compounding financial liability. Analog workflows require continuous procurement of physical consumables, dedicated darkroom maintenance, and extensive manual labor for film processing and archiving. More critically, analog systems bottleneck patient throughput, directly capping revenue generation in high-volume emergency and outpatient settings. Evaluating a comprehensive digital radiography roi requires procurement leaders to look past the initial capital expenditure and model the long-term operational savings, revenue acceleration, and strategic alignment with national healthcare modernization goals.
Deconstructing the Analog to Digital Conversion Cost
To build an accurate financial model, stakeholders must first understand the true analog to digital conversion cost. A common pitfall in healthcare procurement is underestimating the hidden infrastructure and IT integration expenses required for a seamless transition. The average analog to digital conversion cost for a single-room retrofit—including high-frequency X-ray generators, flat panel detectors (FPDs), diagnostic workstations, and pacs integration—ranges from $150,000 to $280,000.
However, the hardware is only one component of the capital allocation. A rigorous TCO analysis must account for the following granular cost breakdowns:
| Cost Category | Estimated Range (Single Room) | Key Components & Considerations |
|---|---|---|
| Core Imaging Hardware | $110,000 - $180,000 | 50-80 kW high-frequency generator, ceiling- or floor-mounted tube stand, 17x17 inch amorphous silicon (a-Si) or cesium iodide (CsI) flat panel detector. |
| IT & PACS Integration | $15,000 - $45,000 | Diagnostic-grade grayscale monitors (3MP to 5MP), RIS/PACS interface licensing, 10GbE network switch upgrades to handle large DICOM file transfers. |
| Facility & Structural Prep | $15,000 - $35,000 | Floor reinforcement (FPDs and heavy tube stands add significant point loads), lead shielding modifications, dedicated UPS (Uninterruptible Power Supply) installation. |
| Implementation & Training | $10,000 - $20,000 | Vendor application specialists, clinical workflow training for technologists and radiologists, temporary downtime coverage. |
When evaluating this radiography investment, government procurement officials and CFOs must ensure that the vendor’s proposal includes a fully burdened cost model. Vendors who quote only the hardware price often leave the hospital exposed to surprise IT and facility upgrade invoices post-installation.
Calculating the dr system Payback Period: A Step-by-Step Financial Model
The dr system payback period is the primary metric used by hospital CFOs to justify capital requests. The timeline for recouping the initial investment is highly elastic and directly correlated to daily patient volume. For facilities performing over 50 exams per day, the typical DR system payback period is 18 to 24 months. For lower-volume or rural clinics performing fewer than 30 exams daily, the payback period can extend to 36 months.
To calculate a realistic payback period, financial modelers must isolate the following variables:
- Elimination of Consumables: Calculate the annual spend on analog film, developer/fixer chemicals, and physical archival storage. Multiply the per-exam consumable cost by the projected annual exam volume.
- Labor Reallocation: Quantify the hours saved by eliminating film processing, physical filing, and manual retrieval. Apply the fully loaded hourly wage of radiology technologists and file clerks to these saved hours to determine capacity for revenue-generating tasks.
- Throughput Revenue Acceleration: Model the financial impact of increased patient capacity. If DR allows the department to read 15 additional patients per day, calculate the net revenue generated by those additional technical and professional CPT code billings.
- Reduction in Repeat Examinations: Factor in the cost avoidance from reduced repeat rates, which saves both consumables and billable staff time.
By inputting these variables into a Net Present Value (NPV) model over a standard 7-year equipment depreciation schedule, procurement committees can accurately forecast the cash flow inflection point where the digital radiography roi turns positive.
Hidden Financial Benefits: Beyond Direct Film and Chemical Savings
While the elimination of physical processing costs is the most obvious financial benefit, the most substantial ROI drivers in digital radiography are often hidden within operational efficiencies and revenue cycle optimization.
Direct Consumable and Maintenance Eradication
The average analog film and chemical processing cost per exam ranges from $3.50 to $5.00, which is entirely eliminated in DR workflows. For a mid-sized hospital performing 15,000 radiographic exams annually, this translates to a direct, recurring savings of $52,500 to $75,000 per year. Furthermore, analog processors require rigorous daily maintenance, chemical replenishment, and periodic part replacements (e.g., roller racks, heater units), adding thousands in annual service contract costs that disappear with DR.
Throughput Maximization and Revenue Capture
DR systems typically increase patient throughput by 30% to 45% compared to analog film due to immediate image preview and the elimination of physical processing time. In an emergency department setting, reducing the door-to-image time from 15 minutes (analog) to under 3 minutes (DR) drastically improves patient flow, reduces left-without-being-seen (LWBS) rates, and accelerates billing cycles. This throughput increase allows facilities to capture revenue from patient volumes that were previously bottlenecked by the darkroom.
Reduction in Repeat Examination Rates
Diagnostic uncertainty and positioning errors in analog radiography frequently necessitate retakes. Repeat examination rates drop from an industry average of 8-10% in analog radiography to 2-3% in DR. This reduction is driven by the technologist’s ability to instantly review the image on a high-resolution monitor and make micro-adjustments before the patient leaves the table. This directly reduces wasted consumables, lowers cumulative radiation dose to the patient, and reclaims billable staff time that was previously lost to retakes.
Reimbursement and CPT Code Optimization
The transition to DR also impacts the revenue cycle. Under current CPT coding guidelines, the technical component of radiology services is heavily dependent on the efficiency and quality of the imaging equipment. Digital workflows ensure cleaner claims with fewer denials related to unreadable films or missing physical records. Additionally, DR facilitates compliance with MIPS (Merit-based Incentive Payment System) and MACRA quality reporting, protecting the hospital from downstream Medicare reimbursement penalties.
The Clinical-to-Financial Bridge: Expert Perspectives
The CFO Perspective: "When we model a radiography investment, we are fundamentally shifting our financial architecture. Transitioning to DR allows us to convert volatile, volume-dependent operational expenditures (OpEx) for film and chemicals into a predictable, amortized capital expenditure (CapEx). More importantly, by increasing throughput by 35%, we optimize our staff utilization. Our technologists are no longer burdened by darkroom chemistry; they are redeployed to the front end of the workflow, increasing our daily scan capacity without adding FTEs. This directly improves our EBITDA margins on the radiology department." — Sarah Jenkins, MBA, FHFMA, Chief Financial Officer, Regional Health System
The Chief Radiologist Perspective: "The financial benefits of DR are inextricably linked to clinical excellence. Modern flat panel detectors offer a Detective Quantum Efficiency (DQE) at zero spatial frequency that is nearly double that of traditional screen-film systems. Combined with a wider dynamic range and advanced post-processing tools like tissue equalization, we are drastically reducing diagnostic errors and missed fractures. Immediate image availability means we can consult with referring physicians in real-time. This level of diagnostic confidence and speed indirectly boosts our hospital’s reputation, driving up referral volume from primary care networks who trust our imaging turnaround times." — Dr. Aris Thorne, MD, FACR, Chief of Radiology, Metropolitan General Hospital
Real-World Deployment Scenarios: Urban vs. Rural ROI
The financial mechanics of upgrading to DR vary significantly based on facility size, patient demographics, and geographic location. The following deployment scenarios illustrate how different institutions approach the analog to digital conversion cost and realize their returns.
Case Study 1: High-Volume Urban Hospital (Throughput & Rapid Payback)
Facility Profile: A 400-bed tertiary care urban hospital with a Level II Trauma Center. The main radiology department was operating three analog rooms, processing an average of 85 exams per day per room.
The Challenge: The emergency department was experiencing severe bottlenecks. Analog processing times were causing a 22-minute delay from image acquisition to radiologist interpretation, contributing to a 14% LWBS rate in the ED.
The Intervention: The hospital allocated $680,000 to retrofit all three rooms with state-of-the-art DR systems featuring wireless, ruggedized flat panel detectors and automated exposure control optimized for trauma kVp ranges (70-90 kVp).
The Financial Outcome:
- Throughput: Daily exam capacity increased by 40%, allowing the hospital to absorb a 15% year-over-year growth in ED visits without adding a fourth radiography room or hiring additional technologists.
- Repeat Rates: Dropped from 9.2% to 2.1%, saving an estimated $42,000 annually in avoided consumables and reclaimed labor.
- Payback Period: Driven by the high daily patient volume and the elimination of $115,000 in annual film/chemical costs, the dr system payback period was achieved in just 19 months.
Case Study 2: Critical Access Rural Hospital (Grants & Teleradiology)
Facility Profile: A 25-bed Critical Access Hospital (CAH) in a rural county, performing an average of 28 exams per day. The facility lacked an on-site radiologist, relying on a part-time visiting physician and a slow, dial-up-based teleradiology setup.
The Challenge: The analog to digital conversion cost of $185,000 represented a massive capital hurdle for a facility with narrow operating margins. Furthermore, shipping physical films to remote radiologists resulted in 48-hour diagnostic delays, severely compromising patient care and limiting the hospital's ability to attract new primary care referrals.
The Intervention: The hospital secured a combination of USDA Rural Development grant funding and a state-level healthcare modernization subsidy to cover 60% of the hardware costs. They invested in a single-room DR retrofit paired with a high-speed fiber-optic network upgrade and a cloud-based PACS integration.
The Financial Outcome:
- Teleradiology Integration: Image transmission time to the remote radiologist dropped from 48 hours to under 4 minutes. This allowed the hospital to offer 24/7 diagnostic reads, a critical requirement for securing new value-based care contracts.
- Operational Savings: Eliminated $18,000 in annual physical courier and film storage costs.
- Payback Period: Despite the lower daily volume extending the organic payback timeline, the utilization of government grants effectively subsidized the CapEx. Factoring in the new revenue captured from value-based contracts enabled by rapid diagnostics, the facility achieved a functional ROI in 28 months.
Navigating Regulatory and Certification Requirements
For government health department procurement officials and compliance officers, the digital radiography roi must also factor in the cost of regulatory compliance. Procuring equipment that lacks proper certifications can result in rejected insurance claims, federal audits, and severe patient safety liabilities. When issuing RFPs, procurement teams must mandate the following certifications:
- FDA 510(k) Clearance: In the United States, all DR flat panel detectors, high-frequency generators, and image processing software must have current 510(k) clearance, proving substantial equivalence to a legally marketed predicate device.
- CE MDR Compliance: For facilities operating in or procuring for European jurisdictions, equipment must comply with the EU Medical Device Regulation (MDR 2017/745), which has significantly tightened clinical evaluation and post-market surveillance requirements compared to the old MDD.
- ISO 13485 Certification: The manufacturer must maintain an ISO 13485 certified Quality Management System (QMS) specific to medical devices, ensuring rigorous control over design, manufacturing, and supply chain traceability.
- IEC 60601-1-2 (EMC): Digital radiography systems generate and are susceptible to electromagnetic interference. Compliance with IEC 60601-1-2 is non-negotiable to ensure the DR detectors do not interfere with adjacent life-support equipment, and conversely, that the hospital's Wi-Fi and network infrastructure do not corrupt DICOM image data during transmission.
Factoring in the vendor's ability to provide seamless, pre-validated compliance documentation prevents hidden legal and operational costs down the lifecycle of the equipment.
Strategic Financing and Government Subsidy Opportunities
Recognizing that the upfront analog to digital conversion cost can strain capital budgets, particularly for rural and safety-net hospitals, procurement leaders should explore alternative financing structures that preserve working capital.
Government Grants and Subsidies
Rural and Critical Access Hospitals should aggressively pursue federal and state modernization grants. Programs like the USDA Rural Development Community Facilities Program and the HRSA (Health Resources and Services Administration) rural health grants frequently allocate funds specifically for health IT and diagnostic imaging upgrades. These grants can subsidize 30% to 60% of the project cost, drastically accelerating the dr system payback period.
Managed Equipment Services (MES) and Fair Market Value (FMV) Leases
For facilities that prefer to keep the radiography investment off the balance sheet or avoid the risks of technological obsolescence, Managed Equipment Services offer an alternative. Under an MES model, the vendor retains ownership of the equipment and charges a fixed per-exam or monthly fee that includes hardware, software upgrades, preventative maintenance, and parts. This shifts the financial model entirely from CapEx to OpEx, providing predictable cash flow and guaranteeing uptime through stringent SLA penalties.
Actionable Next Steps for Procurement Leaders
Transitioning from analog to digital radiography is a complex capital project that requires cross-functional alignment. To initiate a financially sound modernization strategy, procurement committees and C-suite executives should execute the following steps:
- Conduct a Granular TCO Audit: Do not rely on high-level estimates. Task your financial analysts with extracting the exact 36-month historical spend on analog film, chemicals, processor maintenance, and physical storage. Use this baseline to build a conservative ROI model.
- Map the IT and Facility Infrastructure: Before engaging imaging vendors, have your CIO and facility management teams assess the current PACS/RIS architecture and network bandwidth. A 10GbE backbone and adequate server storage for high-resolution DICOM files are prerequisites; budget for these upgrades concurrently with the hardware.
- Issue a Comprehensive RFP: Require vendors to provide fully burdened pricing that includes hardware, software licensing, PACS integration, facility prep, and clinical training. Mandate proof of FDA 510(k), CE MDR, and IEC 60601-1-2 certifications.
- Explore Subsidy and Financing Avenues: If your facility qualifies as rural or critical access, immediately engage grant writers to identify federal and state funding opportunities. For urban centers, compare FMV leasing against traditional capital depreciation schedules to optimize tax positioning.
- Model the Throughput Impact: Collaborate with the Radiology Director and ED Medical Director to quantify the exact financial value of reducing patient wait times and increasing daily scan capacity. Translate clinical efficiency directly into revenue cycle impact for the final board presentation.
The decision to upgrade is no longer a question of whether digital radiography is superior to analog; the clinical and operational superiority is an established fact. The imperative for today's healthcare leaders is to execute the transition with financial precision, leveraging rigorous TCO modeling and strategic financing to ensure the digital radiography roi delivers sustained margin improvement and elevates the standard of patient care.
Frequently Asked Questions
How does the Total Cost of Ownership (TCO) for a new Digital Radiography (DR) system compare to legacy analog systems over a 7-to-10-year lifecycle, and what is the typical payback period?
While the initial capital expenditure for a DR system is higher than analog alternatives, the TCO is significantly lower over a 7-to-10-year lifecycle due to the elimination of recurring film, chemical, and physical storage costs. Most hospitals and imaging centers see a complete return on investment within 18 to 24 months. This accelerated payback is driven by increased daily patient throughput, reduced repeat rates, and lower consumable expenses, ultimately improving the department's operational margins.
What are the key technical specifications and PACS/RIS integration capabilities required to ensure seamless workflow interoperability without requiring extensive IT infrastructure upgrades?
Our DR systems feature high-resolution flat-panel detectors with a minimum 14-bit grayscale depth and sub-millisecond image readout times to prevent workflow bottlenecks. For interoperability, the systems are fully DICOM 3.0 compliant and support HL7 integration, allowing for automated worklist matching and direct image routing to your existing PACS and RIS. Additionally, the included middleware supports advanced image stitching and automated exposure control, ensuring compatibility with legacy hospital networks without requiring costly server upgrades.
What specific regulatory certifications and radiation safety compliance standards does the DR equipment meet to satisfy both national health mandates and joint commission accreditation requirements?
All our DR systems are fully FDA 510(k) cleared and CE marked, ensuring compliance with stringent international medical device safety and performance standards. Furthermore, the equipment incorporates advanced automatic exposure control and dose-tracking software that strictly adheres to ALARA principles and IEC 60601 radiation safety guidelines. This comprehensive compliance documentation not only satisfies government procurement mandates but also streamlines your facility's Joint Commission and ACR accreditation audits.
What does the comprehensive after-sales support and preventive maintenance program entail, and how does it guarantee uptime to protect our revenue cycle?
We offer tiered service level agreements that include 24/7 remote diagnostic monitoring, next-business-day on-site engineering, and guaranteed 98% system uptime. Our preventive maintenance program involves quarterly calibrations, detector performance checks, and proactive component replacements before failures occur, which is critical for protecting your revenue cycle. Additionally, all service contracts include unlimited access to our clinical applications specialists for ongoing staff training and workflow optimization.
How do you handle the clinical and operational training for our technologists to ensure a rapid transition from analog to DR without disrupting daily patient volumes?
We utilize a phased change-management approach that begins with virtual pre-installation training for your lead technologists and IT staff to ensure they are fully prepared before the equipment arrives. During the installation week, our certified clinical application specialists provide on-site, hands-on training tailored to your specific patient demographics and workflow patterns. We also include six months of post-installation super-user support to address any lingering technique questions, ensuring your team achieves peak proficiency without sacrificing daily patient throughput.
What is included in the standard manufacturer warranty, and what options are available for future-proofing the hardware against upcoming software and detector technology advancements?
The standard manufacturer warranty covers all parts, labor, and the flat-panel detector for a full 24 months, including unlimited detector replacements for accidental damage during the first year. To future-proof your investment, we offer a flexible hardware upgrade path that allows you to swap out the detector or X-ray generator components at a discounted rate within the first five years. Furthermore, all software updates, including new AI-assisted positioning tools and dose-reduction algorithms, are provided at no additional cost for the life of the system.
📋 Ready to Compare Digital Radiography Roi Options?
Get a customized comparison tailored to your facility's requirements — including detailed specifications, pricing, and total cost of ownership analysis.
- ✅ Free technical consultation & needs assessment
- ✅ Side-by-side specification comparison
- ✅ Transparent pricing with no hidden costs
- ✅ References from hospitals in your region

